psychiatry 1. definition of major depression : if 5 out of 9 symptoms persist for more than 2 weeks symptoms can be remembered with mnemonics: low mood SIGECAPS S-sleep I-loss of interest G-guilty/ worthlessness E-lack of energy C- concentration/ attention A-Appetite loss P-psychomotor changes S-suicidality Low mood In adjustment disorder, the precipitant can be anything except bereavement. what is the difference between normal grief vs major depression? In normal grief about the death of a loved one, the idea ruminates around that loved one only. she may think she would have died with her loved ones. She can feel auditory/visual hallucinations of her loved ones. But these do not significantly impair daily life functioning. these episodes occur intermittently but in major depression, these symptoms are persistent. In major depression, there is greater social and occupational dysfunction. 2. How to differentiate schizoaffective disorder from mood disorder with psychotic feat...
Posts
Treatment of ADHD first-line treatment is drugs in children aged 6 and above. In children below 6 years, the first line of treatment is behavioral therapy. Among drugs, first, try stimulants (amphetamine/ methylphenidate). Second-line options are atomoxetine and clonidine. what is the mechanism of action of atomoxetine norepinephrine reuptake inhibitor How to titrate the dose of the stimulant? we should titrate it every week until max dose is reached or the patient experiences intolerable side effects. H ow long to wait to see whether the stimulant will be effective? its effect is seen within 1 week. if the patient does not feel improvement within 1 week, change to alternate medications. what are the features of stimulant toxicity? diaphoresis, mydriasis, tachycardia, hypertension, dilated pupil, anxiety, agitation, psychosis, decreased appetite cannabis intoxication also causes tachycardia, and hypertension; then how to differentiate it from stimulant toxicity? in cannabis ...
Difference between serotonin syndrome (SS) and neurolept malignant syndrome (NMS): in SS, a patient has neuromuscular hyperactivity (hyperreflexia, myoclonus, ocular clonus) instead of bradykinesia and rigidity in NMS. Fluoxetine has a half-life of 5 weeks, so, before switching to MAOi, wait for 5 weeks because it will cause serotonin syndrome.
HPV vaccination in boys/ girls: Vaccination at 9-12 years of age (if missed then can take till 26 years of age) what are the conditions where it can be given after 26 years of age? answer: HCPs who are involved in surgery of HPV wounds; people who have not been previously exposed to HPV due to few sexual partners schedule of vaccination: under 15 years of age: 2 vaccinations at 6 months apart if the age is more than 15 years or immunocompromised patients, give 3 vaccination: 0, 1-2month and 6 month
Ethics practice in medicine 1. if any colleague is doing substance abuse, this must be reported to the state licensing board because the primary aim is to maintain patient safety. 2. if any patient gives a gift to a physician with some expectation that he will give me preference, do not accept the gift. otherwise, physicians can accept inexpensive gifts. 3. if any intoxicated patient comes to the ER and needs emergency treatment but the patient denies treatment, then sedate him and do an investigation and treatment. Because the patient is not currently in a state of being able to make the correct decision. so, assume that his decision will be further treatment and go ahead without consent.
Health insurance system in the USA 1. Medicare 2. Medicaid 3. Medicare-Medicaid (Medi-Medi) 4. Medigap (medicare supplemental insurance) Medicare: it is for people aged more than 65; physically or mentally disabled, with end-stage renal disease, and only certain neurodegenerative diseases (e.g. amyotrophic lateral sclerosis). It has 4 parts: A, B, C, D part A covers inpatient services part B covers outpatient services, outpatient surgery, and preventive care. part C (medicare advantage): this is provided by private insurance companies and it includes both inpatient and outpatient expenses PART D covers prescription drugs Medi-medi includes very low-income seniors, disabled who qualify for both Medicare and Medicaid. Medigap covers expenses not covered by parts A, B, and D. It covers copays and deductibles.
How to distinguish CSF findings whether it is a traumatic lumbar puncture or subarachnoid hemorrhage? if xanthochromia (degenerated RBC) is present, it is due to subarachnoid hemorrhage because it takes more than 2 hours for the degeneration of RBC. If frank blood is present then the RBC: WBC ratio is 700 -1000: 1
function of lobes of the cerebrum: nondominant parietal lobe: constructional apraxia, dressing apraxia Dominant parietal lobe: acalculia, inability to recognize fingers, inability to write, inability to identify or distinguish left/ right side of body. nondominant temporal lobe: impaired perception of complex sounds (auditory agnosia) Dominant temporal lobe: difficulty expressing their thoughts in a meaningful manner, Wernicke aphasia
Hungry bone syndrome it occurs between 2-4 days after parathyroidectomy. initially, when PTH was high, there was an outflux of calcium from bone into the blood. After parathyroidectomy, calcium starts to influx into the bone. serum calcium falls to nadir between 2-4 days postoperatively. what are the risk factors for Hungary bone syndrome? severe hyperparathyroidism, vitamin D deficiency, and severe bone disease. All these conditions have a high bone turnover rate.

Brainstem infarction pons is divided into mid pons and inferior pons; lateral side and medial side. This division is based on blood supply. infarction of medial pons causes ataxic hemiparesis (contralateral hemiparesis of limbs and ipsilateral paresis of facial muscles and ataxia due to involvement of middle cerebellar peduncle). There may also be a loss of sensation of touch and position sense. Infarction of lateral part of mid pons causes involvement of sensory and motor division of cranial nerve five (weakness of masticatory muscles, diminished jaw jerk) Infarction of the lateral part of the inferior pons causes involvement of cranial nerves seven and eight. Infarction of the medial part of medulla oblongata causes alternate hypoglossal hemiplegia (tongue deviates toward the side of the lesion and limb paresis occurs on the opposite side). there is also a loss of vibration and proprioception on the contralateral side. Infarction of the lateral part of medulla oblongata causes H...
CRANIAL TUMORS Pinealoma: vertical gaze palsy, loss of optokinetic nystagmus and pupil reflex, ataxia headache due to obstructive hydrocephalus Some pineal tumors are germinoma and secrete hcg which can cause precocious puberty in prepubertal males. craniopharyngioma: associated with diabetes inspidus and absence of one or more pituitary hormones. Frontal lobe tumor associated with Foster-Kennedy syndrome (optic atrophy on the side of the tumor and papilledema on the contralateral side)
Brain death First of all, rule out confounding factors: major endocrine and electrolyte disturbances, drug intoxication, hemodynamic instability (core body temperature should be greater than 36 degrees C, Systolic BP more than 100 mm Hg) apnea test: disconnect the ventilator for 10 minutes and let PaCo2 rise to 60mm Hg (or above 20mm Hg from baseline) and pH fall to less than 7.28, if the patient is not able to initiate their own breath, then the apnea test is positive. absence of brainstem and cerebral reflexes e.g. pupil, gag, tracheal suction reflex, caloric reflex, dolls eye reflex, extensor posturing
some conditions of pregnancy where extra prophylaxis is required pre-eclampsia Risk factors of pre-eclampsia High risk: DM, hypertension, CKD, autoimmune disease, multiple gestation, prior preeclampsia Moderate risk: obesity, advanced maternal age, nulliparity prophylaxis: aspirin beginning at 12 week period of gestation preterm labor: if the cervix is less than 2cm, then vaginal progesterone if a history of preterm labor, then give intramuscular hydroxyprogesterone prevention of neural tube defect in the general population, 0.4mg of folic acid if high risk of neural tube defect (e.g. prior neural tube defect, carbamazepine, valproate), then give 4mg folic acid
Rh incompatibility in pregnancy lets us understand this with a case scenario: a female with 28 weeks of gestation (POG) presented to you for follow-up. She is Rh-ve; Rh's status of her father is unknown because he is out of contact. At 8 weeks of POG, she had chorionic hematoma for which she received anti-D immunoglobulin. This time, her lab report says that her anti-D immunoglobulin status is negative. Does she require anti-D immunoglobulin this time? Yes, she requires it now and postpartum as well. when there was a chorionic hematoma, blood from the fetus entered the mother. To neutralize that, she received anti-D immunoglobulin. This time, her antibody status is negative means that she did not form much immunoglobulin against the exposed blood of the fetus. So, she requires again immunoglobulin at 28 weeks of gestation to protect her from future bleeding during delivery. let us say, at this time, that her anti-D immunoglobulin status would have been positive which means there is...
Group B streptococcal (GBS) infection in pregnancy It is also called streptococcus agalactie. If there is the colonization of this bacteria in the rectum and vagina, there is the possibility of transmission of this bacteria to newborns while delivery. so, if there is colonization, treat it we check with a rectovaginal swab at 35 to 37-week periods of gestation (POG). GBS colonization is transient or intermittent, that's why check at 35-37 weeks POG. Let us take one example to understand this: A female was admitted at 38 weeks of period of gestation because of a rupture of the membrane and labor pain. Her medical history included group B streptococcal colonization at 36-week periods of gestation in her previous pregnancy. At that time, she was treated with IV penicillin. Does this time also, require penicillin? The answer is: In this case, we do not know the colonization status of her in this pregnancy. so, we need to wait for 18 hours in this case. If she does not deliver b...
HERBAL SUPPLEMENTS 1. BLACK COHOSH: it has been promoted for the treatment of post-menopausal symptoms. it causes hypotension, adverse estrogenic effects, and hepatotoxicity. 2. LICORICE: it contains glycyrrhenetic acid, which inhibits the conversion of cortisol to cortisone. it is used for viral infections/ bronchitis, and stomach ulcer. 3. Ginkgo biloba: it has been marketed as an anti-oxidant, used for memory enhancement. it is also used in dementia, macular degeneration, and peripheral vascular disease. Adverse effects include increased bleeding, especially in people taking aspirin. 4. Ginseng: it is also used for memory enhancement. Side effects include increased bleeding. 5. saw palmetto: it is used for the treatment of Benign prostate hyperplasia. Its adverse effects include mild stomach discomfort and increased bleeding risk 6. St John wort: It has been marketed for use in mild to moderate depression and insomnia. it is also used as an anti-inflammatory and wound healing. ...
Acute epididymitis causative bacteria: gonorrhea and chlamydia if the age is less than 35 while coliform bacteria in a person aged more than 35. clinical features epididymitis may be associated with urethritis causing urethral discharge and pain at the tip of the penis relief of pain with scrotal elevation investigation : urine R/E M/E, urine c/s; NAAT for gonorrhea/ chlamydia if age is less than 35. Treatment: if gonorrhea is suspected: ceftriaxone+ doxycycline if gonorrhea is less likely, then fluoroquinolones (levofloxacin) supportive measures: scrotal elevation, NSAIDs
Pregnancy How much exercise to do in pregnancy? 30 min of moderate-intensity exercise. Do as much so that you can have a conversation while exercising. If a patient has already adapted to high-intensity exercise for a long time, then she can continue it during pregnancy. The following types of activities are not recommended in pregnancy. 1. scuba diving, sky diving: due to risk of fetal decompression sickness from an air embolus formation. 2. contact sport 3. exercise with a falling risk (e.g. skiing, gymnastics, horseback riding etc). 4. exercise with marked training, resistance training, Valsalva maneuver
HEPATITIS B If a child is born of a mother/ father with Hep B, give Ig plus HBV vaccine within 72h, then give normal HBV vaccine series (0, 2,6 months). obtain HBsAg serology 3 months after the last vaccine (at 9 months of age). They advise to get serology between 9-12 months. If you check it early, it can be a false positive and if you check after 12 months, it can be a false negative because titer decreases with time.

Foodborne illness scombroid poisoning : this occurs if seafood is not stored at a temperature below 15 degrees Celsius. That is why histidine in these foods gets converted to histamine. so, when a person eats this food, he gets histaminergic symptoms that are self-limited. Such symptoms include flushing, throbbing headache, palpitation, abdominal cramps, diarrhea, and oral burning. These types of features manifest within 10-30 minutes after eating. A person may complain of a bitter taste while eating. On physical examination, a physician may find skin erythema, wheezing, tachycardia, and hypotension pufferfish poisoning that causes neurological symptoms e.g. perioral tingling, incoordination, and weakness.
skin lesions due to fungus Histoplasmosis : It primarily affects the lungs but it can also affect the skin if it is disseminated. If it is disseminated, the patient will be ill-looking coccidioidomycosis : It also primarily affects the lungs but can also cause skin abscess Sporotrichosis : it is common in landscapers, and gardeners because it is transmitted from the soil, and decaying plants. at the site of inoculation, first of all, a papule appears that progresses to ulceration and subsequently travels along the lymphatic chain. From the ulcer, there can be a discharge of odorless (serous ) fluid Treatment: 3-6 months of oral Itraconazole Blastomycosis also primarily affects the lungs but it can affect skin. in the skin, you will see verrucous lesions with heaped-up borders.
viral infections in children Roseola infantum : it is caused by human herpes virus 6. In this condition, the rash appears once fever disappears. The rash begins on the neck/ trunk and is uncommon on the palms. coxsackie virus : it causes 1. hand, foot, and mouth disease and 2. herpangina. In herpangina, the ulcer is on the posterior oropharynx while it is in the anterior aspect in hand, foot, and mouth disease How to distinguish whether vesicles on hand are caused by herpes (herpetic whitlow) vs Coxsackie? in hand, foot, and mouth disease, vesicles are present on bilateral hands while it is unilateral in herpes. Lesions on the hand appear after autoinoculation from the mouth.
Diabetic foot ulcer How to do diagnosis? if you probe the wound and the probe hits the bone, it means that the patient has developed osteomyelitis. This "probe to bone test" has the highest specificity for the diagnosis of osteomyelitis. But if this test is negative, then you have to do an x-ray or MRI. MRI has the highest sensitivity among imaging modalities followed by a 3-phase bone scan. X-ray has the least sensitivity among all tests for diagnosis of osteomyelitis. CT scan also can be done but it is a less sensitive test than MRI. if metal hardware interferes with MRI, then a nuclear scan (3-phase bone scan, tagged WBC scan) is done. Let us say, there is one patient with a diabetic foot ulcer and underlying osteomyelitis. you had taken a wound swab and it revealed 3 bacteria with antibiotic sensitivity reports. Now, the question is can we rely that the same bacteria is causing osteomyelitis or the bacteria on the superficial might be contaminant as well? The answer is ...
congenital infections Congenital rubella Congenital CMV Congenital toxoplasmosis Similarities Sensorineural hearing loss, purpuric lesions, hepatosplenomegaly difference Blueberry muffin rash, Cataract, Patent ductus arteriosus, microcephaly, low birth weight Periventricular calcification Intracerebral calcification

vibrio vulnificus and mycobacterium marinum what are the similarities and differences between them? similarities: both are transmitted from water (e.g. fish tank, sea) both cause cellulitis Differences: vibrio vulnificus causes rapidly progressive ulceration, and necrosis (within 12 hours) while a lesion of Mycobacterium marinum takes 72 hours to develop. vibrio vulnificus causes necrotizing and bullous lesions while Mycobacterium marinum causes papular and ulcerative lesions. vibrio vulnificus is transmitted by ingestion and wound contamination while mycobacterium marinum gets contracted with wound contamination. Treatment of vibrio vulnificus: ceftriaxone plus doxycycline

Oral ulcers and pharyngitis in children 1. Herpangina: It is an infection caused by the Coxsackie virus in children. Generally, it occurs in the summer season. There are painful vesicles on the posterior pharynx, and tonsillar pillars causing painful pharyngitis. children can present with painful drooling, decreased appetite, and headaches. Handwashing prevents the spread of this virus. 2. Group A streptococcal pharyngitis: tonsillar exudates and anterior cervical lymphadenopathy 3. Herpes gingivostomatitis: vesicles and ulcers on the anterior oral mucosa and around the mouth. Fever can be present. 4. apthous stomatitis: ulcer on anterior oral mucosa
post-exposure prophylaxis in HIV Fluids with a high risk of infectivity include blood, blood containing body fluids, semen, vaginal secretions, and fluids with a possible risk of infectivity including pericardial fluid, pleural fluid, synovial fluid, CSF, and amniotic fluid. Body fluids such as urine, feces, vomitus, and tears are noninfectious unless they contain visible blood in them. what kind of injury is at risk of infection? breached skin mucus membrane e.g. eye percutaneous injury to the skin Treatment is 3 anti-retroviral drugs for 4 weeks. start it as soon as possible.
screening of colon cancer: in the general population, they tell to start screening at 50 years of age with the following methods: 1. colonoscopy and repeat every 10 year 2. guaiac fecal occult blood test or fecal immunochemical test (FIT) every year 3. FIT DNA every 1-3 year 4. CT Colonography every 5 years. 5. flexible sigmoidoscopy every 5 years and if combined with FIT, do 10 yearly In a person with a family history of colon cancer start screening at 40 years of age or 10 years earlier whichever comes first and then repeat every 3-5 years. whom to consider family history positive? Before answering this question, first, let us talk about what is an advanced adenomatous polyp is. Advanced polyp means either size of polyp more than 1 cm villous or high-grade dysplasia Now see the definition of family history below: 1. if First degree relative with colon cancer or advanced adenomatous polyp diag...
Dysphagia we need to distinguish whether it is oropharyngeal dysphagia or esophageal dysphagia because our investigation of choice will be different. How to distinguish by clinical features? In oropharyngeal dysphagia, there is difficulty initiating swallow and drooling, aspiration, and cough for oropharyngeal dysphagia or dysphagia due to upper esophageal pathology, UGI endoscopy is not helpful because when u insert the endoscope from the upper esophagus, it can miss it. That's why, we prefer a nasopharyngeal laryngoscope (NPL) or barium esophagogram.
Stress ulcer prophylaxis Indication: if any 1 of the following: 1. coagulopathy ( PT INR >1.5, APTT more than 2 times ULN, platelet <50,000 2. spinal cord injury, head trauma, major burns 3. mechanical ventilation for more than 48 hours 4. GI bleeding or ulceration in the last 12 months if any 2 of the following: 1. ICU stay for more than 7 days ...
upper gi bleeding causes: 1. splenic vein thrombosis Etiology: Acute or chronic pancreatitis, pancreatic cancer clinical features: The difference between isolated splenic vein thrombosis and portal hypertension is that there are isolated gastric varices in splenic vein thrombosis but both gastroesophageal and gastric varices are present in portal hypertension. Treatment for patients with splenic vein thrombosis and GI bleeding is splenectomy. 2. Hepatic veno-occlusive disease : there is occlusion of terminal hepatic venules (not veins) that causes post-sinusoidal portal hypertension. Etiology: most commonly occurs in patients with bone marrow transplant clinical features: tender hepatomegaly, jaundice, ascites.
massive blood in stool in elderly patients Two major causes are: 1. Diverticular bleeding: It occurs due to the eroding of a small artery of the colon. Bleeding is often self-limited but it can recur. 2. Angiodysplasia Risk factors include aortic stenosis, End-stage renal disease, and von Willebrand disease.
pancreatitis Drugs causing pancreatitis: 1. diuretics: thiazide, furosemide 2. anti-hypertensive: enalapril, Losartan 3. immunosuppressants: cyclosporine 4. antibiotics: Metronidazole, tetracycline, trimethoprim-sulfamethoxazole, isoniazid 5. antivirals: lamivudine, didanosine 6. anti-epileptics: valproate, carbamazepine 7. analgesics: NSAID, acetaminophen, mesalamine, sulfasalzine, opiates 8. others: asparaginase, estrogen, sertraline
when to suspect Ectopic pregnancy? If beta-hcg is more than 1500 and you are not able to detect an intrauterine gestational sac, it means it is ectopic pregnancy. in normal pregnancy, beta-hcg rises by more than 35% every 48 hours. if it is not rising in this trend, suspect ectopic pregnancy. Do you know that bleeding can occur during implantation as well? After 2 weeks of fertilization or 4 weeks of the last menstrual period, there is scant bleeding due to the attachment of the fertilized egg to the uterine lining. what is a corpus luteal cyst? when implantation inside the uterus occurs, it is a physiological cyst that produces progesterone to maintain intrauterine pregnancy.

Imperforate hymen It results from failure of canalization of the lower third of the vaginal plate during the development A neonate can have mucocolpos (mucus accumulation in the vagina causing bulging of the hymen) or this condition may not be diagnosed in childhood unless a female presents at 13-14 years of age when she undergoes menarche. Then menstruating blood accumulates in the vagina but cannot come outside (primary amenorrhea) because the hymen is intact, thus it causes bluish bulging outside (this is called hematocolpos). She can experience cyclical abdominal pain, weight loss, and loss of appetite. She can experience constipation due to compression symptoms. Since Hymen is not perforated, she has retrograde menstruation, which means blood flows in the fallopian tube which then spills into the peritoneal cavity causing intraabdominal adhesions. on examination, we can find tender suprapubic mass due to blood accumulation in the uterus causing uterine enlargement...
Breast lump Benign Breast lump In adolescence, it can be fibroadenoma and fibrocystic changes while at the age of 35-50s, it can be a breast cyst. what are the differences and similarities between fibroadenoma and fibrocystic changes? in both conditions, pain occurs before the onset of menses. The difference is that fibroadenoma is a unilateral, single rubbery lump while fibrocystic changes are bilateral, multiple, and generalized small masses. pain in fibroadenoma is unilateral while in fibrocystic changes, it is bilateral. what is the treatment of fibroadenoma? Fibroadenoma regresses spontaneously after a few months. if it is persistent, then do USG to evaluate. what is a breast cyst? it occurs at the age of 35-50s. it is a tender, solitary mass that resolves after aspiration. Evaluation of breast mass : if the age is less than 30, then do USG. if the age is more than 30, then do Mammography. Mammography cannot delineate mass in young females aged less than 30 because of dense b...
Likelihood ratio Definition: positive likelihood ratio (+LR) it is how likely the test is positive in a diseased population when you compare the positive test in a non-diseased population. +LR= positive test in a diseased population/ positive test in a non-diseased population Negative likelihood ratio (-LR) it is how likely the test is in a diseased population to be negative when you compare it to a negative test in a nondiseased population. -LR= negative test in diseased population/ negative test in nondiseased population. How to interpret the likelihood ratio (LR)? the higher the LR, we can rule in disease and the lower the LR, we can rule out disease. LR 2 increases the probability of disease by 15%, LR 5 increases the probability of disease by 30%, and LR 10 increases the probability of disease by 45% On the contrary, LR 0.5 decreases disease probability by 15%, LR 0.2 decreases it by 30% and it is decreased by 45 % if LR is 0.1 LR 0.1 is strong evidence to rule ou...


primary amenorrhea: when to evaluate? lack of menstruation by 15 year of age if secondary sexual characteristics are present and by age 13 if those are absent. EVALUATION OF PRIMARY AMENORRHOEA initial tests: beta hcg, TSH, Prolactin, pelvic Usg I like to mention here one of the cases I had seen in my clinical practice. A mother of a 15-year-old girl brought her daughter for evaluation of primary amenorrhea. on examination, she had developed breasts but no axillary and pubic hair. I sent for usg pelvis which revealed no uterus. Then I sent serum testosterone and FSH. The report revealed normal male levels of serum testosterone and normal FSH. her possibility was androgen insensitivity syndrome because she had an absence of axillary and pubic hair. In addition, she had normal male serum testosterone levels. Due to these reasons, mullerian agenesis was unlikely because in mullerian anomaly, there is a normal female serum testosterone level and there should have been the presence of axil...

PUBERTAL DEVELOPMENT puberty in girls Breast development (thelarche) occurs at 8-12 years of age and menarche occurs 2 years later. Growth spurt occurs shortly before menarche. It is abnormal if a girl does not start menstruating at the age of 15 and needs to be investigated. we should investigate primary amenorrhea at the age of 13 if a girl has not developed secondary sexual characteristics (breast, axillary, and pubic hair) Delayed puberty At 14 years of age in boys, the testicular volume should be at least 4 ml; if it is less than that, it suggests hypogonadism. it can be either primary or secondary hypogonadism. a. primary hypogonadism: Klinefelter syndrome b. secondary hypogonadism: Kallmann syndrome, craniopharyngioma, chronic malnutrition, stress, hypothyroidism, hyperprolactinemia How to differentiate hypogonadism from constitutional delay? In x-ray, in both conditions, bone age lags behind chronological age and lagging of development of secondary sexual character...
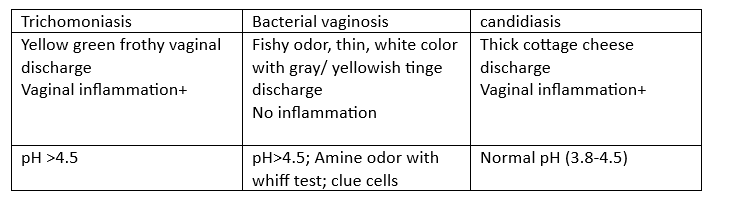
PELVIC INFLAMMATORY DISEASE (PID) and STI in female Risk factors: 1. Multiple sexual partners: this is the biggest risk factor. It increases risk by 5 to 20 times 2. previous PID 3. Not using barrier contraceptives 4. age group of 15-25 years old because there is a high risk of gonorrhea and chlamydia in this population. Treatment: on OPD patients, we use ceftriaxone+ doxycycline In Inpatient, we use cefoxitin+ doxycycline. clinical features and investigation findings in vaginal discharge

contraceptives 1. OCP : Nowadays, low-dose estrogen OCP is available. Due to the low estrogen component, there can be breakthrough bleeding (irregular bleeding). The mechanism of irregular bleeding is that the endometrium gets thinned with low estrogen. so, to prevent that high doses of estrogen can be given during periods of breakthrough bleeding. A common myth is that OCP causes weight gain which is not true. During the initiation of OCP, a person can experience breast tenderness, moodiness, headache, and nausea which subside after some time. OCP also helps to improve acne, and hirsutism in PCOS and decrease the risk of endometrial and ovarian cancer. Absolute contraindication of combined hormonal contraceptives: a. migraine with aura b. age 35 and above who smoke more than 15 cigarettes /day c. coronary artery disease/ stroke d. thromboembolic disease e. anti-phospholipid syndrome f....

1. How do medication, other physiological conditions like pregnancy, and pathological conditions like acute hepatitis and chronic liver disease affect thyroid hormone metabolism and the requirement of levothyroxine if the patient is already on thyroid supplements? There are some proteins in blood like thyroxine-binding globulin (TBG) that transport levothyroxine (T3, T4) In blood to peripheral tissue. pregnancy, acute hepatitis, oral contraceptive pills containing estrogen, and medications like tamoxifen, and raloxifene increase TBG. When TBG rises in the blood, TBG binds to free T3 and free T4 increasing the total T3, and T4 in the blood and decreasing the concentration of free T3, and free T4. Peripheral tissue senses the low level of free T3, and free T4, thus it stimulates the pituitary gland to produce more TSH. TSH in turn stimulates the thyroid gland to produce free T3 and free T4. 2. what are conditions where TBG decreases? a. chronic liver disease b. drugs like androgenic horm...